
Quick answer: Tetanus is a serious bacterial infection that enters the body through a wound and causes painful muscle stiffness and spasms, most recognizably “lockjaw.” It is now rare and highly preventable with the tetanus vaccine; after an injury, a booster is generally recommended if your last shot was over 5 years ago for a dirty wound, or over 10 years for a clean one.
Parents ask about tetanus far more often than pediatric cases occur. That is not a bad thing. It means the DTaP vaccine is doing its job. The CDC counts fewer than 30 cases a year in the entire United States. Most are in adults who lost track of their boosters. Pediatric cases are so rare that many pediatricians go a full career without seeing one.
The questions parents ask are reasonable. A child stepped on something. A toddler is due for the next DTaP and a parent is reading about side effects online. An older kid hasn’t had a shot in eight years and just got a bad cut at soccer. These are good questions, and the answers are not as complicated as the internet often makes them sound.
So instead of writing a textbook entry on tetanus, I want to do something more useful: answer the questions parents commonly ask, in the order they tend to come up.
How does someone actually get tetanus?

The bacteria that causes tetanus, Clostridium tetani, lives everywhere: soil, dust, animal manure. You cannot avoid the bacteria. What matters is the toxin it produces. The bacteria only make that toxin when conditions are right. Deep, low-oxygen, and sealed off. A long scrape that bleeds freely is actually much safer than a small puncture that closes over and seals shut.
This is the part most parents have backward. Size of the wound matters less than its shape and what is in it. A clean kitchen knife cut is almost never a tetanus risk. A barely visible splinter in a garden that was recently manured is exactly the kind of wound the CDC built its booster guidance around.
Two things worth putting to rest while we are here. Tetanus is not contagious. Your child cannot catch it from a sibling or a classmate, because it does not spread person to person. And rust itself does not cause tetanus. Rusty objects come up because they tend to be old, outdoor, and dirty, so they are more likely to carry the bacteria. The rust is a marker, not a cause.
For the CDC’s overview: Tetanus: For Parents and Caregivers.
When does my child need a shot after a wound?

This is one of the most common questions parents ask. The honest answer depends on two things: what kind of wound it is, and how long since the last shot.
For a clean, minor wound (a shallow cut, a scrape, the kind of injury you would normally handle at home), your child is protected if their last DTaP or Tdap was within the past ten years. If it has been longer than ten, a booster is recommended.
For a deeper or dirtier wound (a puncture, an animal bite, a glass cut, a contaminated burn, anything involving soil or manure), the window is shorter. Up to five years since the last shot, no booster needed. Beyond five years, get the booster.
A few situations need a clinician’s eye regardless of timing:
- Children under seven who have not completed the DTaP series
- Children whose immunization records are missing or unclear
- Severely contaminated wounds, including animal bites
- Crush injuries with significant tissue damage
- Burns covering a large area
If you do not know when the last shot was, and many parents do not, that is not a reason to guess. Contact your child’s pediatrician, previous pediatrician, state immunization registry, or school health office to locate the record. A clinician who provides pediatric care can then determine whether a booster or further evaluation is appropriate.
Basic wound care at home
For most cuts and scrapes, the steps are simple:
- Stop the bleeding with firm pressure using a clean cloth.
- Rinse the wound under cool running water. Use mild soap on the skin around it, not in the wound itself.
- Remove visible dirt or debris if it comes out easily. Leave anything deep or embedded for medical evaluation.
- Apply an antibiotic ointment and cover with a clean bandage.
- Watch for increasing redness, warmth, swelling, pus, or red streaks over the next two to three days.
Seek prompt evaluation from your child’s pediatrician or urgent care if the wound is deep or wide, an animal or human bit your child, something is embedded, the wound is on the face or hand or over a joint, you cannot fully clean it, or your child is not up to date on tetanus shots. None of these are emergencies in the 911 sense, but they are reasons to be seen the same day.
For the CDC’s full wound-care guidance: Tetanus Prevention After Injury.
What is in the shot, and how often does my child need one?
The DTaP vaccine protects against three diseases at once: diphtheria, tetanus, and pertussis (whooping cough). The CDC schedule has been stable for years and works well.
| Age | Vaccine | Why this dose |
|---|---|---|
| 2 months | DTaP (dose 1) | First exposure, starts building immunity |
| 4 months | DTaP (dose 2) | Reinforces the response |
| 6 months | DTaP (dose 3) | Strengthens further |
| 15-18 months | DTaP (dose 4) | First real booster |
| 4-6 years | DTaP (dose 5) | Pre-kindergarten booster |
| 11-12 years | Tdap | Adolescent booster, especially important for pertussis |
| Every 10 years after | Td or Tdap | Adult booster cycle |
A few things worth knowing about this schedule. The early doses build the initial immunity. The body needs the repeated exposures, spaced months apart, to develop a strong response. The pre-kindergarten dose tops off protection before school. The adolescent Tdap exists partly because pertussis immunity fades faster than tetanus immunity does, and the booster catches both.
If your child missed a dose or started the schedule late, that is not unusual and it is fixable. The CDC publishes a catch-up schedule that adjusts the timing. Your child’s pediatrician can use the CDC catch-up schedule to determine the appropriate timing.
What about side effects of the tetanus vaccine?
Most side effects of DTaP and Tdap are mild and resolve on their own within two to three days. The most common: soreness at the injection site, mild redness or swelling, low-grade fever, and fussiness in younger children. These usually start within the first 24 hours.
A few less common reactions worth recognizing:
- After the fourth or fifth DTaP dose, some children develop noticeable swelling of the arm or leg where the shot was given. It looks worse than it is and resolves on its own.
- Very rarely, a child cries inconsolably for more than three hours after the shot. This is uncommon, distressing, and almost always resolves without complications. Tell your pediatrician at the next visit.
- Severe allergic reactions (hives, swelling of the face or throat, or difficulty breathing within minutes of the shot) are extremely rare but require immediate emergency care. This is the one situation that calls for 911.
For common side effects, age-appropriate acetaminophen or ibuprofen effectively manages fever and soreness. Do not give aspirin to children. A cool compress on the injection site helps.
One thing I want to address directly because it comes up often. DTaP and Tdap safety data are among the best studied in pediatric medicine. Decades of surveillance through VAERS and the Vaccine Safety Datalink consistently confirm the side-effect profile above. If you have concerns (a previous reaction, an allergy, or a family history), discuss them with the clinician who will administer the vaccine before the appointment so they can review your child’s history and explain the options.
For more from the CDC: DTaP and Tdap Vaccine Safety.
What does tetanus actually look like? When do I rush in?

I want to handle this section carefully because the goal is recognition, not anxiety.
Symptoms typically appear three to twenty-one days after the bacteria enter the body, with most cases developing within seven to ten days. Shorter incubation periods often mean more severe disease.
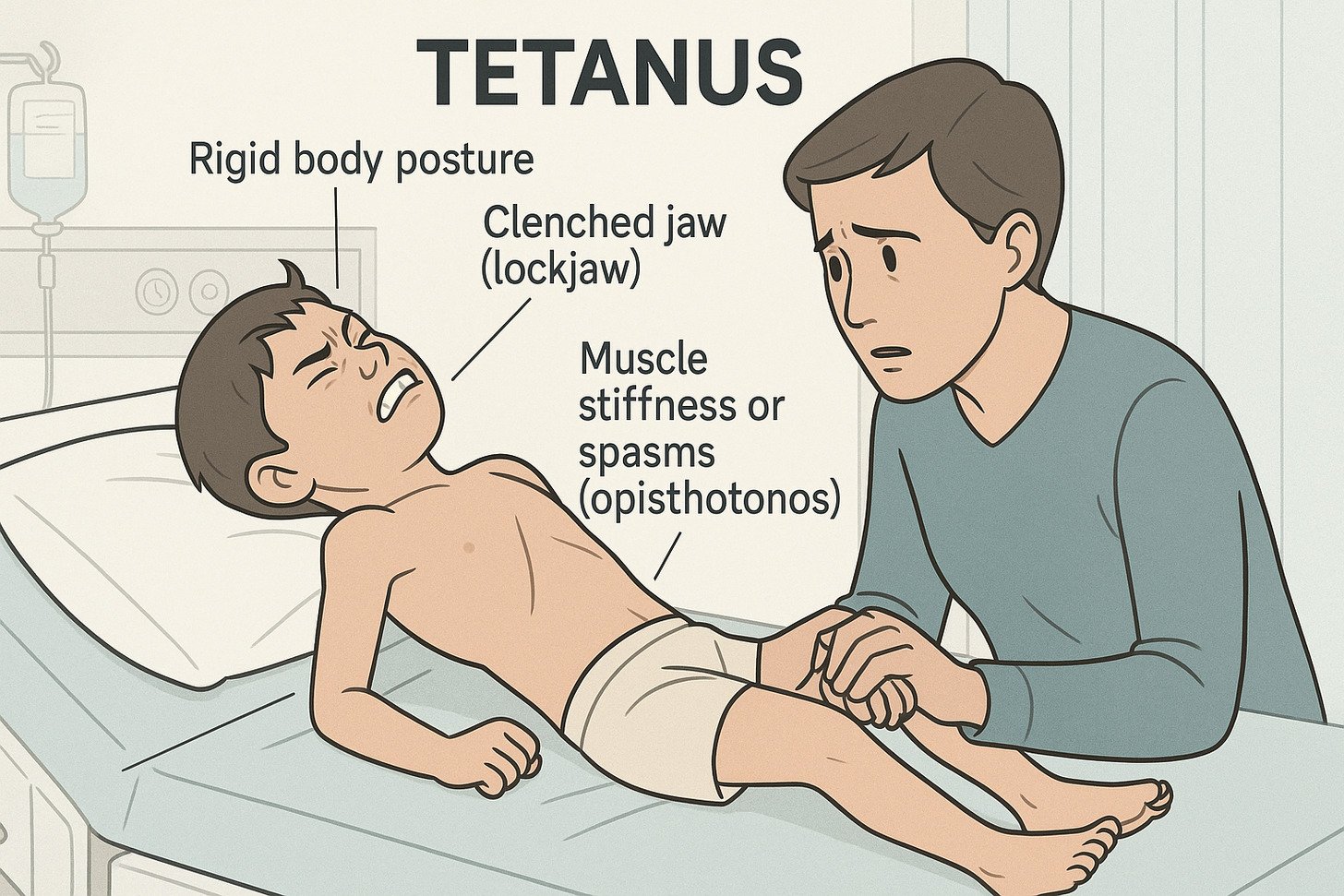
The earliest sign is usually jaw stiffness. The muscle that controls opening the mouth tightens and resists. That is where the nickname “lockjaw” comes from. Neck stiffness and difficulty swallowing tend to follow.
Early signs to watch for
- Jaw stiffness or difficulty opening the mouth
- Painful muscle spasms in the face and neck
- Difficulty swallowing
- Irritability and restlessness
- Headache and low-grade fever
Advanced symptoms
- Painful muscle contractions throughout the body
- Rigid abdominal muscles
- Arching of the back (called opisthotonus)
- Seizures or convulsions
- Changes in blood pressure and heart rate
When tetanus becomes a medical emergency
Without prompt treatment, tetanus can cause respiratory failure from breathing muscle spasms, aspiration pneumonia, fractures from severe spasms, and heart rhythm problems. The case fatality rate is real, which is why the CDC and the American Academy of Pediatrics treat tetanus as a medical emergency.
If your child has any of these symptoms after a wound (jaw stiffness, neck stiffness, muscle spasms), go to the emergency department or call 911 immediately. Treatment requires hospitalization and antitoxin. Outcomes are dramatically better the earlier it starts.
I want to be clear about something, though. Most jaw soreness in children is not tetanus. Most stiff necks in children are not tetanus. The combination that should trigger concern: under-vaccinated child, plus a recent wound, plus these specific symptoms. If you are unsure, contact your child’s pediatrician or urgent care for guidance.
Common questions parents ask about tetanus
“My child stepped on a nail. Do they need a shot tonight?”
A nail puncture should be assessed using the wound type and your child’s vaccination history. Rinse the wound with clean running water and contact your child’s pediatrician or urgent care promptly, especially if the wound is deep, dirty, or contains debris. Do not wait for symptoms to decide whether the wound or vaccination status needs evaluation.
“We can’t find the immunization records.”
Start with the previous pediatrician’s office, your state’s immunization registry, or the school health office. If records cannot be located, a pediatric clinician can use the CDC catch-up schedule and the wound history to determine the appropriate next step. Do not guess or restart a vaccine series without clinical guidance.
“My child is afraid of the shot.”
A real thing, and worth taking seriously. There are practical techniques that help: positioning, distraction, a topical numbing cream applied 30 to 60 minutes before, and the order of injections when multiple shots are given. Ask the vaccination provider about these options before the appointment so the team has time to prepare. A few minutes of preparation makes a meaningful difference.
“Can my child get tetanus from a cat or dog scratch?”
The scratch itself is less the issue than what was on the animal’s claws or in the saliva. Animal bites carry a higher risk of tetanus than scratches, and any animal bite that breaks the skin should be evaluated for tetanus risk, rabies risk, and routine wound infection. Contact your child’s pediatrician or urgent care rather than waiting for symptoms.
“Is the tetanus shot safe during pregnancy?”
Yes, and recommended. Tdap is given during the third trimester of every pregnancy, typically between 27 and 36 weeks, to protect both the mother and to pass antibodies to the newborn before their own DTaP series begins. This is one of the strongest protections we have for infants in their first months.
Special situations worth knowing about
Children with incomplete vaccination. Catch-up immunization is straightforward in most cases. A pediatric clinician can build a catch-up schedule based on your child’s age and documented doses. The CDC’s catch-up tables are practical and well-tested.
Tetanus immune globulin (TIG). For an unvaccinated or under-vaccinated child with a high-risk wound, doctors sometimes administer TIG alongside the tetanus shot. TIG provides immediate short-term protection while the vaccine takes effect. This is a hospital or urgent-care decision, not a home one.
International travel. Children traveling to regions with limited medical care need current tetanus shots before departure. In some destinations, access to TIG or sterile wound care may be limited. Prevention matters even more. If there is a gap in your child’s records and a trip is coming up, ask for an expedited catch-up plan.
When and where should parents seek care?

If your child has a deep, dirty, or contaminated wound and their tetanus vaccination status is not clearly current, contact their pediatrician or urgent care promptly. If they show possible tetanus symptoms after a wound, such as jaw stiffness, neck stiffness, or muscle spasms, go to the emergency department or call 911. Questions about vaccine schedules, side effects, or wound-specific decisions should go to the clinician responsible for your child’s care.
Educational scope: Savera Wellness does not provide pediatric vaccination, immunization-record review, catch-up scheduling, or wound-treatment services. This article provides general education only. For advice about a specific child or wound, contact the child’s pediatrician, vaccination provider, urgent care, or emergency services as appropriate.
This article is for general education and does not provide medical advice, diagnosis, or treatment. Savera Wellness does not provide pediatric vaccination or wound-treatment services. Contact your child’s healthcare professional for individual guidance. For a medical emergency, call 911.
Medically reviewed by Dr. Meenu Vaid, MD — Board-certified in Internal Medicine, Infectious Disease, and Addiction Medicine. Last reviewed on June 27, 2026.
Related: Rabies vs Tetanus: What Makes These Infections Different?
Medically reviewed by Dr. Meenu Vaid, MD, Board-Certified in Internal Medicine and Infectious Disease. Last clinically reviewed on August 2, 2026.
This article is for general educational purposes only and is not medical advice. Reading it does not create a doctor-patient relationship. For emergencies call 911. For crisis support call or text 988. Read our full medical disclaimer.



One Response
Insightful post! Your clear explanations of tetanus risks in children and simple prevention tips especially clean wound care and vaccines are highly valuable.